Bonnie asks, What the heck is a herniated brain, anyhow?
And I resist the temptation to reply, A brain that's not working very well any more.
Although that's basically it. Herniation is a condition where your brain gets squooshed out of position by increased intracranial pressure. A lot of things can cause that increase in ICP: stroke, tumor, hemorrhage, blunt injury, you name it. Some of those things can be stopped easily before the brain squooshes too far; others are trickier to fix.
There are actually six different ways your brain can squoosh inconveniently. Those ways are divided into two groups: the supratentorial and the infratentorial. The name "-tentorial" comes from an anatomical landmark; what you need to know is that there are four ways of squooshing the brain up high and two of squooshing it down low. And, you know, that it's...deadly, unless you stop it and fix it.
Herniation is thankfully pretty rare. Your brain can take a lot before it moves so far to one side or the other, or downward or upward, that structures actually get crushed and torn and you die. Plus, a lot of things happen *prior* to things getting to that point that clue the average observer in that Things Aren't Right. That's not to say that herniation doesn't happen suddenly--it can, and I've seen it--but thankfully, that's not all that common.
Now, on to Celeste's question, which is something along the lines of What up with all the amnesiacs in the daytime soaps, yo? Wouldn't all these people be running around with severe neurological injuries if they had amnesia this often in real life?
Celeste has, as we say in the business, hit it on the head. Amnesia is indeed very rare and is accompanied either by a pretty complex neurological injury (some strokes can do it, to varying degrees) or by a physiological and psychological disorder called "conversion disorder".
Now, this doesn't mean that people with amnesia are either completely gorked or crazy. I would point you to Oliver Sacks, who writes interesting stories about patients of his who had perfectly intact distant memories, but who couldn't form new ones. That's a type of amnesia. There are other types that wipe out middle-range memory or even old memories. It all depends on what hits your brain where. Thankfully--again--this is really rare, partly because the brain is amazingly tough, and partly because we have all these neat redundant systems built into it.
Conversion disorder is a little trickier. It's something that's normally dealt with by both psychiatrists and neurologists, because there are components of the syndrome that have to be handled in different ways. Horribly oversimplified, conversion disorder is the body's response to extreme stress. You get sick in one way or another, or have a traumatic event happen, and as you're coming out of it, you suddenly start getting sicker in weirder ways than anybody ever thought possible.
This is not malingering, and the people with CD aren't crazy. It's not something like Munchausen, where the person is actively trying to make himself sick. Instead, the protective functions of the brain and body kick in overactively in an attempt to protect the person. (Amnesia is considered one of the rarest manifestations of CD; I've seen it exactly once.) When it starts to happen, it's frightening and often more debilitating than the original insult to the person was.
And finally, to Crowscalling's question: How the heck is that speech-bulb thingy supposed to function?
To answer that question, I'm going to have to share with you some of the crash course in oral and oropharyngeal anatomy I've gotten in the last few weeks.
Look at your mouth. Now look at mine. Now back to your...shit, sorry. I turned over two pages at once.
Okay. Look at your mouth. You see how you've got a nice bony palate in the front and a nice flexible one in the back? Those help you make specific consonant sounds, like "K" and "L" and "M" and even "S" and "B". You'd be surprised how much happens at the back of your throat when you talk.
When you lose that nice flexible dome-shaped soft palate and/or the structures that make up the back of your throat, two things happen: First, you can't say "B" (comes out more like "M") or any number of other things. And, you sound like Fran Drescher gone crazy, because there's so much air escaping through your nose. "Hypernasality" is how they describe it formally; that's sort of like calling the ocean "moist".
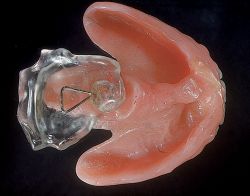
A speech bulb is something about the size and shape of...oh, heck, I dunno...a chicken drummette, like you'd get in a wings bucket? Or maybe the first joint of your thumb? Anyway, it's not huge, but it's not petite. It's job is to sit up in the back of your throat and cover any holes there, and also cover any holes in your soft palate. That way you can sound almost completely normal right away. It moves the airflow from your sinuses to out of your piehole, and it gives your tongue and throat something to press and move against to form words.
You wouldn't think a little chunk of plastic would do all that, but it is AMAZING.
(Which makes me wonder: If I spoke French, or German, or, Frog help me, Danish with all its back-of-the-throat Rs and stuff, would my speech bulb be shaped differently? Must remember to ask Dr. DDS.)
And thus endeth the latest edition of You Ask, I'll Oversimplify! Further questions--on any topic, not just neuroscience or speech bulbs or my current favorite toenail polish--are welcome in the comments.





{kind=link}